A 28/F WITH VOMITINGS AND SHORTNESS OF BREATH
This is an online e log book to discuss our patient de-identified health data shared after taking his / her / guardians signed informed consent. Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.
This E blog also reflects my patient centered online learning portfolio and your valuable inputs on the comment box is welcome.
I have been given this case to solve in an attempt to understand the topic of " patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with diagnosis and treatment plan. is an online e log book to discuss our patient de-identified health data shared after taking his / her / guardians signed informed consent. Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.
A 28 year old female resident of Nalgonda presented to hospital with
CHIEF COMPLAINTS:
-Vomitings since 10 days.
-Burning micturition since 10 days.
-shortness of breath since 2 days.
HISTORY OF PRESENTING ILLNESS:
Patient was apparently asymptomatic 10 days ago when she developed vomitings,6-8 episodes per day,non projectile,non bilious,non blood stained,yellowish to green in colour.There is history of burning micturition since 10 days which got relieved on medication.There is history of pedal edema 10 days ago which had no postural variation and was pitting in type and got relieved spontaneously.There is history of shortness of breath since 2 days,sudden in onset,gradually progressive.
No history of orthopnea,peripheral neuropathy,palpitation,chest pain,loose motions.
PAST HISTORY:
Known case of Type 2 diabetes mellitus since 2 years.
No history of tuberculosis,hypertension,epilepsy,asthma,coronary artery disease.
PERSONAL HISTORY:
-Patient wakes up at 6 am and starts the day with doing her daily chores.
-She eats breakfast like idli,dosa or Upma everyday at 8 am.
-She takes insulin 30 minutes prior to both lunch and dinner and eats rice and curries everyday as meals.
-She is a homemaker and doesn’t have any other physical activity apart from doing daily chores.
-She goes to sleep at 10 pm and doesn’t have disturbed sleep.
-She takes mixed diet,non veg twice weekly and has good appetite.
-Patient has normal bowel and bladder movements,No addictions.
TREATMENT HISTORY:
Insulin 15 units twice daily (30 minutes prior lunch and dinner)
FAMILY HISTORY-
GENERAL PHYSICAL EXAMINATION:
-Patient is conscious, coherent and non cooperative,he is well oriented to time, place, person.
-examined in a well lit area
-moderately built and moderately nourished.
-Pallor-absent
-Icterus- absent
-cyanosis-absent
-clubbing- absent
-lymphadenopathy- absent
-pedal edema- absent
VITALS
Temperature- 98.7 F
Pulse rate- 72 beats per min
Respiratory rate- 29 breaths per minute
Blood pressure -130/80 mm of Hg
SYSTEMIC EXAMINATION
RESPIRATORY SYSTEM
INSPECTION :
-shape of chest normal
- central trachea
-abdomino thoracic type
PALPATION: -
-all inspectory findings are confirmed
PERCUSSION:
-resonant in all areas
AUSCULATION:
-bilateral air entry present
CARDIO VASCULAR SYSTEM :
S1,S2 heard no murmurs heard
PER ABDOMEN
INSPECTION
-all quadrants are moving equally with respiration
-abdominal distention is present,
-umbilicus is inverted, central,
-no scars or sinuses are seen,
- no engorged veins are seen
PALPATION
- all inspectory findings are confirmed
- abdomen is soft
- non tender
- no local rise in temperature,
- no organomegaly is noticed.
PERCUSSION-normal liver span
AUSCULTATION-bowel sounds heard
CNS:
no focal Neurological deficits found
Higher mental functions-normal
Sensory examination-
Right. Left.
Spinothalamic-
Crude touch- normal normal
Pain- normal normal
Temperature- normal normal
Dorsal column
Fine touch Normal. Normal
Vibration.
Medial malleolus 3.5. 4.7
Shaft of tibia 3.6. 5.1
Tibial tuborisity 5.7. 6.0
Cortical
Graphesthesis. Normal normal
Stereognosis. Normal. normal
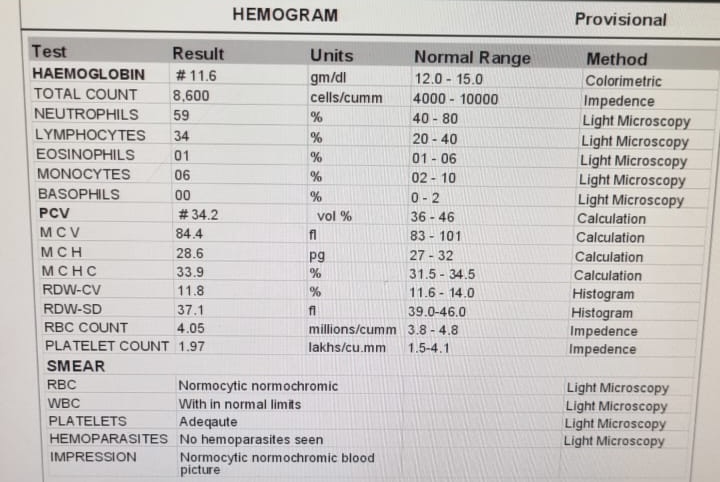
INVESTIGATIONS:






ECG
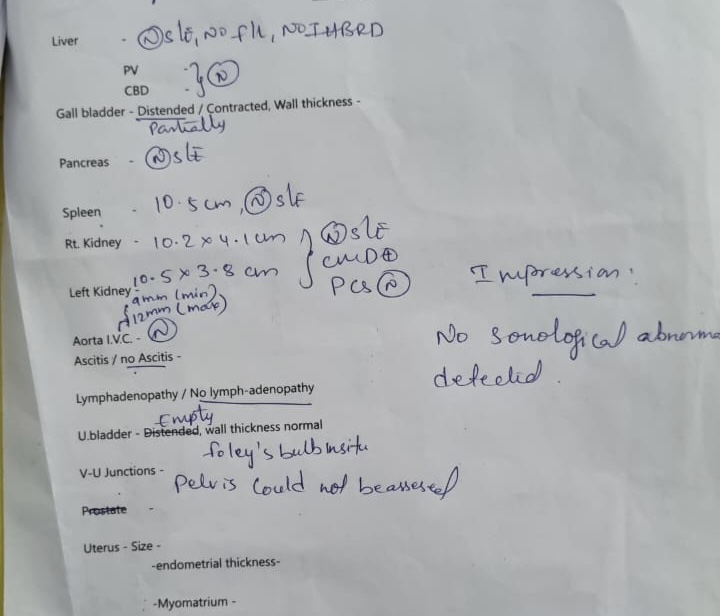
Ultrasound
Provisional diagnosis-DKA

Comments
Post a Comment