66 yr female with abdominal pain, loose motions and generalized weakness
This is an online e log book to discuss our patient de-identified health data shared after taking his / her / guardians signed informed consent. Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.
This E blog also reflects my patient centered online learning portfolio and your valuable inputs on the comment box is welcome
I have been given this case to solve in an attempt to understand the topic of " patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with diagnosis and treatment plan
66 yr old female resident from cherlapally came to opd with chief complaints of
1.Abdominal pain since 2 yrs
2.Loose motions since 2 yrs
3.Generalized weakness since 1 yr
History of presenting illness:
Patient was apparantly asymptomatic 4 yr back then she developed constipation for 1 month ( once in 2 days) which was associated with blood in stool,for which she admitted in hospital and undergone surgery for hemorrhoids.
PAfter 2 yrs she developed loose motions 2-3 times a day which was watery ,mucoid, foul smelling,Non blood stained.It is aggravated by dal and tomato and relieved by taking medication.
History of tenesmus, bloating most oftenly associated after meals
History of abdominal pain in epigastric region which is insidious in onset ,sharp radiating to back.It is aggravated after taking meals and relieved by taking butter milk or medication.
History of generalized weakness since 1 yr
History of nausea and Vomiting (2 episodes per day)intermittently since 10 days which was insidious in onset ,non projectile,non bilious and contents are food particles.It is associated with headache (diffuse type).It is relieved on taking medication.
History of indigestion and heart burn
History of weight loss since 2 yrs
No history of dysphagia, hematemsis,jaundice
No history of hematochezia,melena
No history of fever, cough ,cold .
No history of chest pain , shortness of breath
Past history:
Not a k/c/o DM ,HTN,TB, Asthma, Epilepsy, thyroid disorders
Family history:
No significant family history
Personal history:
Diet : Mixed
Appetite:Normal
Sleep: disturbed
Bowel and bladder movements: Irregular
No addictions
Pallor present


General examination:
Patient is concious,coherent and cooperative
Moderately built and nourished
Temp: afebrile
PR:80 bpm
RR:16cpm
BP: 140/90 mmHg
No icterus ,cyanosis,clubbing,lymphadenopathy and edema
Systemic examination:
Per Abdomen:
Inspection:
Shape - flat
Flanks - free
Umbilicus - inverted
All quadrants moves equally with respiration
No engorged veins, visible pulsations
Hernial orifice are free
Palpation:
No local rise of temperature
Abdomen is soft and non tender
No palpable spleen and liver
No other palpable masses
Percussion:
Resonant
Auscultation:
Normal bowel sounds heard


CVS:
Jvp not raised
Inspection:
Shape of chest - elliptical
No visible pulsations
No engorged veins
Apical impulse not visible
Palpation:
Apex beat present over the left 5th intercostal space medial to midclavicular line
No parasternal heave
No precordial thrill
No dilated veins
Auscultation:
S1 S2 heard ,No murmurs
Respiratory system:
Upper respiratory tarct - normal
Lower respiratory tract:
Inspection:
Chest bilaterally symmetrical,
Shape- elliptical
Trachea- midline
Palpation:
Trachea is central
Normal chest movements
Percussion: in sitting postion
Rt. Lt
Supraclavicular. N(resonant). N
Infraclavicular. N. N
Mammary region. N. N
Axillary region. N. N
Infra axillary region. N. N
Supra scapular region. N N
Interscapular region. N. N.
Infrascapular region. N. N
Auscultation:
Normal vesicular breath sounds
No added sounds
Vocal resonance is normal
CNS :
Higher motor functions - intact
Cranial nerves - intact
Motor system:
Rt- UL. LL. Lt- UL. LL
Bulk - normal N. N. N
Tone - N. N. N. N
Power - 5/5. 5/5. 5/5. 5/5
Reflexes:
UL. LL
Biceps. 2+. 2+
Triceps. 2+. 2+
Supinator. 2+. 2+
Knee 2+. 2+
Ankle. 2+. 2+
Sensory system: intact
Co ordination is present
Gait is normal
No Cerebellar signs
No signs of meningeal irritation
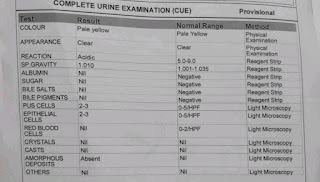
Investigations:











Provisional diagnosis:
Chronic gastritis


Comments
Post a Comment